Priapism
Michael Macias

By Andrew Ketterer & John Sarwark
Let's say you're sitting in your shop when a sharply dressed fifty-somethingish gentleman shuffles in looking very uncomfortable, and also a bit embarrassed. You take your high quality history, and you reveal that he's been using a product known as "Triple Mix", which is a combination of paparavine, phentolamine, and prostaglandin--formulated for the treatment of erectile dysfunction. Specifically, it's meant to be injected into the penis (and amazingly it's FDA approved!).
You discover that he last used said product eight hours ago, and while the treatment was very effective, his erection hasn't gone away, and he's now experiencing some pretty significant pain. You examine him and discover a gloriously tumescent penis. Diagnosis? Priapism! Better get yer gloves on.
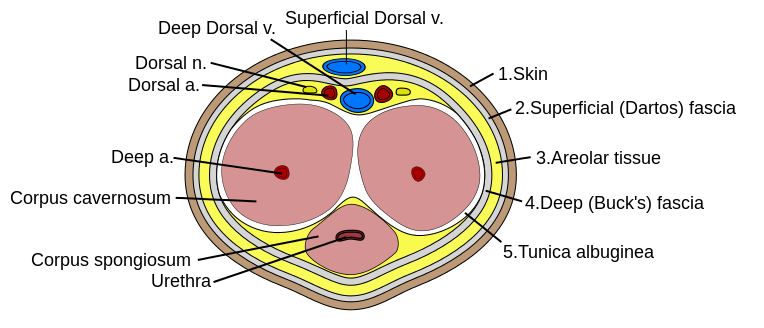
Penis Cross Section Anatomy
Before we do anything, let's start with some basic science review. The erectile tissue of the penis is composed of the cavernosal arteries (the "eyes" of the diagram above), which sit inside the corpora (plural!) cavernosa. An erection occurs when the cavernosal arteries engorge the cavernosa. In normal physiology, this tapers off as cavernosal pressure approaches arterial pressure, until the neuroendocrine system ultimately switches it all off. The blood then drains back out via the emissary veins.
In low-flow priapism (the most common variety), the drainage mechanism gets stuck. This can be caused by compression of the emissary veins (as in iatrogenic cases), venous blockage (seen in sickle cell anemia, leukemia, coagulopathies), or neurohormonal dysregulation (also usually iatrogenic). The far rarer high-flow priapism is caused by uninhibited arterial inflow, and occurs almost exclusively in trauma. Clinically, the hallmark of priapism is a painful erection lasting for several hours in which the glans remains soft and spongy while the corpora remain tumescent.
This can make your patients pretty uncomfortable! What's more concerning is that the priapism can potentially result in ischemia from sludging and clotting in the cavernosa. Irreversible impotence is another possibility. So yeah, it's an emergency, and uh, yeah, you've gotta drain it now.
As it turns out, the procedure is not terribly difficult. You can break it down into a few steps:
Before you poke:
- Start with a warm sitz bath to help dilate the emissary veins and facilitate drainage. At least, this is what Rosen's recommends we start with. Usually pretty futile but it doesn't hurt to try.
- Try peripherally dosing a peripheral vasodilator like terbutaline or hydralazine. These have been quoted as having "variable success."
Once you're ready:
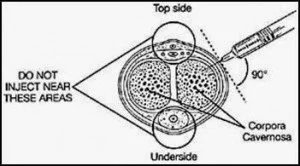
- Anesthetize the skin of the penis with 1 cc or so of lidocaine (WITHOUT EPI!) at approximately 8 o'clock and 4 o' clock on the sides of the proximal shaft. This avoids hitting the dorsal neurovascular bundle and the urethra. You also shouldn't have to go very deep. Note that the image above uses 10 o' clock and 2 o' clock, which is also acceptable. Be generous with this stuff!
- Prior to drainage, attempt detumescence with direct vasoconstrictors. The American Urologic Association recommends phenylephrine at a concentration 100-500 mcg/cc. 1 cc can be injected into alternating corpus cavernosum at the previously anesthetized areas. This can be repeated several times every 3-5 minutes (Lower concentrations should be used in pediatric patients and patients with cardiovascular comorbidities).
- If this fails, your next step is direct drainage. Using sterile technique, stick butterfly needles into the numbed sites, and attach 10 cc syringes to them--smaller syringes will generate better negative pressure. You should be able to evacuate blood immediately. Even if only one side works, there is communication between the corpora, so just keep aspirating.
- If things slow down, try flushing with a few CCs of normal saline through one of the needles. Sometimes you may need to flush into one side while you simultaneously aspirate out the other side
- Drain until detumescence. It will be a bloody mess.
If you get the desired result of detumescence, you should watch your patient for an hour or so to ensure that cavernosal blood doesn't reaccumulate. If they look good after this, the patient can be discharged home with urology follow-up ASAP. If the techniques fail, the patient needs to go to the OR with a urologist--they will need to consider putting in a shunt or excise some clots under anesthesia.
Dr. Larry Mellick has a great demonstration on his YouTube site here:
Some parting pearls of wisdom:
- Ancillary techniques have limited success in improving priapism--you probably just need to drain the thing.
- Drainage is not rocket science, you just need to be sure to avoid poking the dorsal neurovascular bundle as well as the urethra.
- Always be aware of the potential for symptomatic effects of the aforementioned vasoactive substances, especially if the penis is only semi-erect (hint hint -- the emissary veins will carry your phenylephrine downstream).
And as always, these writings and musings are for EDUCATIONAL PURPOSES ONLY. Do we really have to remind you to be careful about going at a penis with a needle? Be safe!
AK/JPS













References
- Roberts and Hedges Clinical Procedures in Emergency Medicine. Saunders 2014, Chapter 55.
- Rosen's Emergency Medicine, Chapter 174.
- The Northwestern Lake Forest Hospital Department of Urologic Surgery
- The American Urological Society Guidelines
- Dr. Larry Mellick's YouTube Page