Not Your Typical Wrist Pain
Michael Macias

Case by Sean Dyer PGY-3 EM Resident; Peer Reviewed by Dr. Christopher Hogrefe, Assistant Professor in Emergency Medicine at Northwestern University Feinberg School of Medicine
The Case
A 32 y/o male presents with wrist pain after being involved in a motor vehicle collision this afternoon. He was holding onto the steering wheel with both hands while at a stop light when his vehicle was struck from behind at approximately 30 miles per hour. His x-ray imaging is seen below:


Diagnosis: Volar Lunate Dislocation
Lunate dislocation is an uncommon traumatic wrist injury that is often a result of high energy trauma from loading of a dorsiflexed wrist along with forced ulnar deviation (i.e holding onto the steering wheel in a rear-end mechanism MVC or falling onto an outstretched hand). The lunate is displaced and rotated volarly (less commonly dorsal rotation), while the remainder of the carpal bones remain in normal alignment relative to the radius. Up to 25% of these injuries can be missed on initial presentation and if left untreated or missed, the function outcome will not be good.
Imaging
AP & lateral wrist x-ray images are useful for making this diagnosis.


On lateral imaging, alignment is lost between the radius, lunate and capitate which can be appreciated by drawing a straight line through these structures. Often, the lunate is seen displaced and angulated volarly, appearing as a 'spilled teacup.'
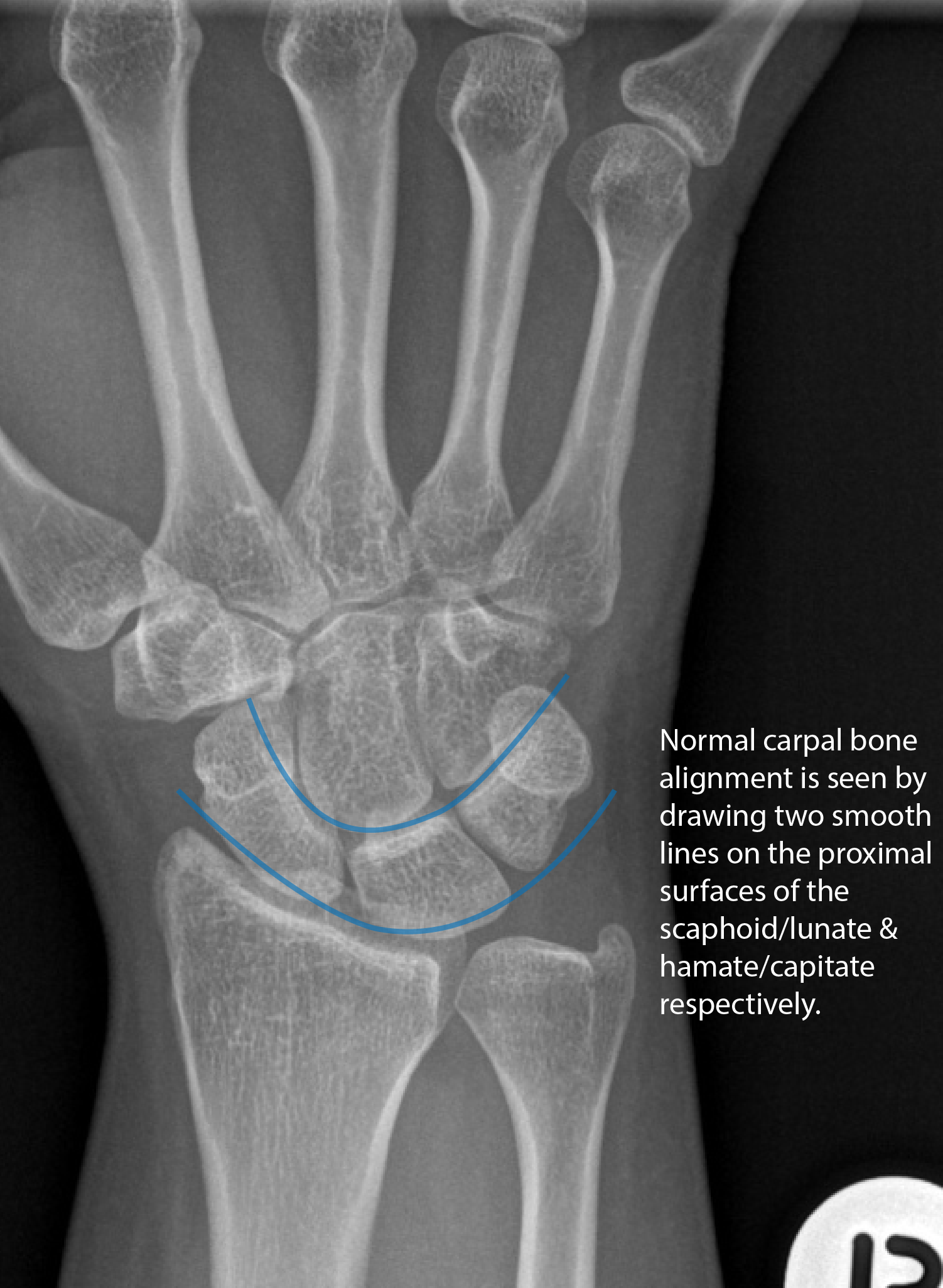

On AP imaging, there is disruption of both smooth lines tracing the proximal articular surfaces of the scaphoid/lunate and hamate/capitate respectively. The lunate is seen overlapping the capitate, triangular (or 'piece of pie') in appearance.
Clinical Exam
Lunate dislocation will commonly present with volar swelling of the wrist and decreased 2-point discrimination to the median nerve distribution. Approximately 25% of patients will display sensory and/or other median nerve symptoms. This is due to acute carpal tunnel. Besides grip strength, be sure to assess the median nerve hand muscle innervation for signs of significant injury:
- L- Lumbricals 1 & 2: Flex MP joints and extend IP joints of thumb and index finger
- O- Opponens pollicis: Allows tip of thumb to touch other fingertips
- A- Abductor pollicis brevis: Allows movement of thumb anteriorly away from palm
- F- Flexor pollicis brevis: Flexes thumb at the MP joint
Management
This injury requires prompt reduction and immobilization in the emergency department. The reduction can be performed with volar pressure and extension of the wrist. After successful reduction, the wrist should be placed in a volar splint. Orthopedic consultation should be obtained from the emergency department as most of these injuries will require surgical repair of the disrupted ligaments. Without surgical intervention, functional outcomes are poor and recurrent dislocation is common. Worst case scenario, avascular necrosis of the lunate can occur, also known as Kienbock disease. Unfortunately even with treatment, many of these patients will still experience future degenerative arthritis.
Important Points
- Lunate dislocation can result in significant chronic pain and loss of function; immediate reduction and orthopedic consultation is warranted in the emergency department.
- This is injury that is often missed by both clinicians and radiologists. Be sure to look at your own films; the lateral wrist x-ray may be the key to your diagnosis.
- Do not confuse this diagnosis for a perilunate dislocation where the radiolunate articulation is preserved and the rest of the carpus is displaced dorsally.
- Given that both lunate and perilunate dislocations are associated with high energy trauma; be vigilant of associated fractures.





References:
- Sherman, S. 2014. Emergency Orthopedics 7th Ed. New York: McGraw-Hill Education
- http://radiopaedia.org/articles/lunate-dislocation
- http://www.orthobullets.com/hand/6045/lunate-dislocation-perilunate-dissociation
- http://www.wheelessonline.com/ortho/perilunate_dislocations