Figure 1 Image of the Week
Michael Macias
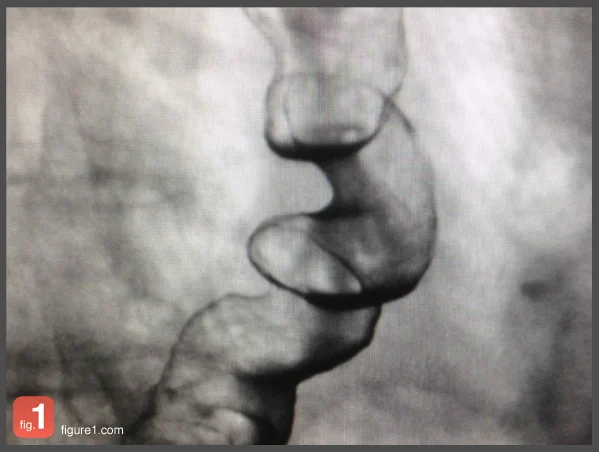
This CSF was drawn from a 26 year-old HIV-positive male who presented
with status epilepticus. The differential diagnosis includes cryptococcal
meningitis, HIV encephalitis, HSV encephalitis, CNS lymphoma, CNS abscess and bacterial meningitis.
See more cases like this on Figure 1.
Laboratory Finding: Xanthochromia
The color of the fluid above is consistent with xanthochromia which refers to the yellow color of the CSF fluid. It is a result of lysis of RBCs and release of pigmented breakdown products such as oxyhemoglobin, bilirubin and methemoglobin. It can also be caused by elevated CSF protein levels, usually greater than 150 mg/dL, from a CNS bacterial or fungal infection. In the right setting, this finding would also be concerning for a subarachnoid hemorrhage.
In many patients with infectious meningitis, the diagnosis is obvious as they present with advanced disease, reporting fever, headache, photophobia, neck stiffness, lethargy, and/or vomiting. However immunocompromised patients and the elderly present a diagnostic challenge and classic symptoms are not often present. A thorough mental status exam is critical in these populations. Physical exam can be useful but often is not. Nuchal rigidity and/or discomfort with neck flexion is common however the classic Kernig's and Brudzinski's signs are of little diagnostic value. Deep tendon reflexex can be increased and ophthalmoplegia may be present, particularly in the lateral rectus muscle.
Starting antibiotics early for the more common culprits such as S. pneumonia, N. meningitidis, & L. monocytogenes is necessary, but also considering other etiologies such as fungal, HSV, or TB in the right circumstance. Once a patient is displaying a focal neurological deficit or active seizure, a CNS abscess or space occupying lesion must be ruled out and a CT scan should be obtained prior to LP. Here is a simple diagnostic-therapeutic work up algorithm for suspected meningitis (click on it to enlarge):
Learn more from FOAMed:
Previous Figure 1 Posts:




References:
Rosen's Emergency Medicine, Central Nervous System Infections.
The color of the fluid above is consistent with xanthochromia which refers to the yellow color of the CSF fluid. It is a result of lysis of RBCs and release of pigmented breakdown products such as oxyhemoglobin, bilirubin and methemoglobin...