Ultrasound Leadership Academy: RUQ Ultrasound
Michael Macias

By Michael Macias
Welcome to the Ultrasound Leadership Academy (ULA) summary blog series. This week, we discuss right upper quadrant (RUQ) ultrasound. The ULA is essentially an online advanced ultrasound education experience put on by the team from Ultrasound Podcast which brings cutting edge learning to emergency medicine personnel through a variety of interactive platforms including video lectures, google hangouts with experts, simulation, live conferences and real time scanning with a pocket-sized ultrasound device known as a Vscan.
Over the next year I will be posting summaries of the key learning points from my experience. If you want to learn more about the program you can visit Ultrasound Leadership Academy or Ultrasound Podcast to see more from the hosts of this awesome program.
Prior to reading this post, I suggest you review our previous post "Introduction to Ultrasound" (including resource links at the bottom of the page) if you are not familiar with the basics of ultrasound.
INTRODUCTION
We all fear the right upper quadrant ultrasound and the elusive gallbladder that often seems to never be in the anatomic space we learned back in medical school. However I am going to convince you that once you learn the basics and a few trouble shooting techniques, it really shouldn't be the the scavenger hunt that you didn't ask for.
The reason we should be performing RUQ ultrasound in the emergency department is multifaceted. Not only does it decreased length of stay(1), it also has the potential to save a significant amount of money by reducing the number of additional radiology studies ordered(2). More importantly, several fairly recent studies have shown that we are good at diagnosing both cholelithiasis and cholecystitis. I have included key tables from a couple studies below with links to original articles included.
You can become proficient in identifying gallstones after 10 scans.
A 2011 systematic review found the pooled sensitivity of emergency physician performed ultrasound for cholelithiasis to be 90%.
Emergency physicians have similar accuracy at detection of acute cholecystitis.
The Anatomy




We have seen the anatomy of the hepatobiliary system many times before but it can still get confusing when looking at it in cross section on ultrasound. Importantly the gallbladder is usually found running along the visceral side of the liver in a transverse plane. It is typically 7-8 cm in length and 2-3 cm in width. Be aware that the gallbladder can take on multiple shapes and be located in different planes as seen in the variant drawing above. Also note that the common bile duct runs together with the portal vein and hepatic artery in the portal triad and lies anterior to the portal vein.
The Technique
Probe: Curvilinear probe (the advantage to this probe is depth however given its large footprint, rib shadowing will be an issue so you will have to keep this in mind)
Positioning: The key to RUQ ultrasound is having proper patient positioning and using the same approach each time. You can choose to start with the patient either completely supine or in the left lateral decubitus. In theory the left lateral decubitus will provide a better view as it helps drop the gallbladder down below the ribs and out from under the liver. If your patient is supine you can also have them take a deep breath in and hold it to move the gallbladder inferiorly for an improved view.
Location: A good starting point is the right costal margin just to the right of midline. Your probe marker should be facing either to the patient's head (sagittal plane) or to the patient's right side. The sagittal technique is usually the preferred initial approach and in this view you will often see the gallbladder in long axis view.
Here is a 1 minute run through of the scan.
The Scan
Identify the gallbladder
Once you have your proper probe, patient positioning, and location, begin to search for a fluid filled structure which should appear hypoechoic with posterior acoustic enhancement. In the sagittal plane you will often identify it in the long axis. Once you do this, rotate your probe 90 degrees to obtain a short axis view and fan through the gallbladder to evaluate for gallstones and gallbladder wall thickening. If you are having trouble finding the gallbladder have the patient take a deep breath in and hold it, or move them to the left lateral decubitus position if supine (or vice versa).
Evaluate for gallstones


Gallstones will appear as echogenic structures with posterior shadowing. They will also be gravitational so when you move the patient they should move accordingly. Large gallstones are fairly easy to see but with small stones you may miss them if you are not looking very closely. Often you may barely see the stone but notice the posterior shadowing so keep an eye out for both when assessing for stones. If you do see a gallstone lodged in the gallbladder neck, you should attempt to turn the patient to see if you can move the gallstone, otherwise this patient may need a surgeon sooner than later. Two caveats to keep in mind:
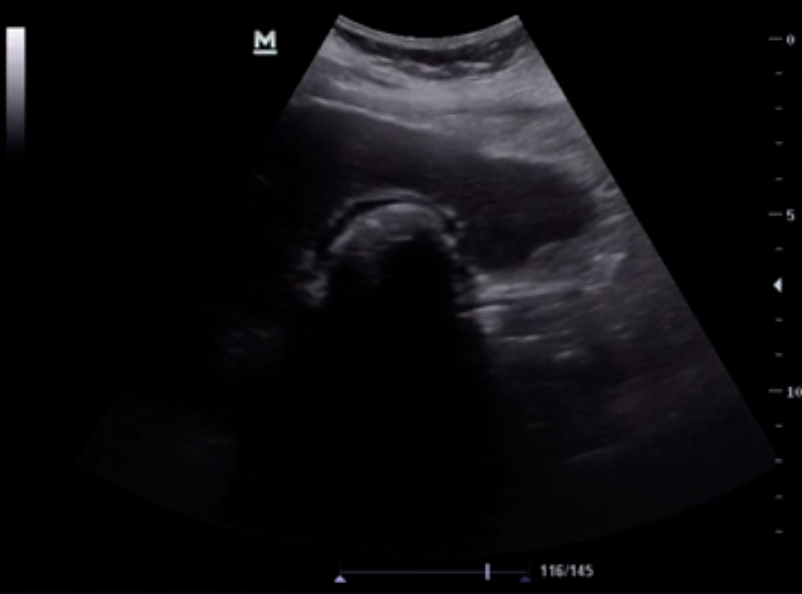
- If you are having difficulty finding the gallbladder and only see a large hyperechoic line with posterior shadowing, this may actually represent a gallbladder that is completely full of gallstones. This is known as the 'wall echo shadow' sign (seen above). So before you say you can't find the gallbladder be sure you aren't missing this finding.
- Gallstones in the gallbladder neck can sometimes be hard to identify as bowel gas shadowing often blends in with the shadowing from the gallstone. Having the patient roll to left or the right can assist with visualization of the stone as it moves via gravity.
Evaluate the gallbladder wall



The gallbladder wall should typically be < 3 mm but some may use 3.5 mm as a cutoff for normal. It is important to always use the anterior wall to measure thickness as this is not obscured by bowel gas. You also should be assessing for pericholecystic fluid around the gallbladder wall which will appear as a thin hypoechoic stripe.
- Be careful when you are assessing the gallbladder wall which appears poorly delineated as this may suggest significant wall edema and false measurement can lead to missed diagnosis of cholecystitis (as seen above).
Find the common bile duct
As briefly mentioned earlier, the common bile duct (CBD) runs together with the portal vein and hepatic artery in the portal triad. It usually runs anteriorly and parallel to the portal vein. Typically the CBD should measure an internal diameter of 2-6 mm. Keep in mind that it does enlarge naturally as we age, so a good rule of them is diameter = 1mm/decade of life.



The first step to finding the CBD is to identify the portal vein as this is the largest of the 3 structures in the triad. You can identify these structures in either the long or short axis. It is often helpful to use the gallbladder neck as a landmark since it will point towards the triad (as seen above). Once you identify the portal vein, apply color doppler or power doppler to identify the portal vein and hepatic artery. The CBD will be the tubular structure superficial to the portal vein in long axis view, or the circular structure in short axis view, without color flow (see image above). 85% of the time the CBD will be the right "ear" on the short axis view but this emphasizes the necessity of color doppler to confirm you are measuring the proper structure.
Essentially what you are looking for in the CBD is dilation. Pathologically, this is usually due to choledocholithiasis, but pancreatic masses and autoimmune disorders can also cause this finding. As we mentioned earlier, normal internal diameter is 2-6 mm (around 1mm/decade of life), and greater than 1 cm is highly sensitive for biliary duct obstruction. However if you do find a CBD that is 7mm and the patient has clinical signs of obstruction to may want to consider consultation.
Is this cholecystitis?
Now that you have evaluated for gallstones, assessed the gallbladder wall and the CBD, you need to decided whether your patient needs to see a surgeon.
- Approximately 85% of patients with cholecystitis will have gallstones (5-14% are acalculous and usually seen in the critically ill) so the lack of gallstones will make the diagnosis less likely.
- Gallbladder wall thickening is specific for cholecystitis but not sensitive, so if you don't see it you cannot rule it out. On the other hand if they do have it you should be very suspicious. (caveat to follow shortly)
- Pericholecystic fluid is not that helpful (similar to a coin flip) but if seen it may push you towards your diagnosis of cholecystitis
- Sonographic Murphy's sign is a very helpful finding (pain when ultrasound probe pressing directly over gallbladder) and this finding with the presence of gallstones has a sensitivity that approaches 90% but has poor specificity. If you have RUQ pain, fever, and elevated WBC count, the specificity of this sign increases significantly to 87%.
- If you have a + sonographic Murphy's sign & gallbladder wall thickening, acute cholecystitis should be on the top of your differential.
There are always caveats. Be sure that when you are evaluating for cholecystitis by ultrasound to not get too honed in on a single finding. Take into account the clinical picture and your patient's other co-morbidities that can skew your findings. Here are just a few conditions that can lead to gallbladder wall thickening in the absence of cholecystitis:
- Ascites
- Heart failure
- Liver failure
- Inflammation (pyelonephritis, PUD, or other intra-abdominal inflammation)
- The 'Big Mac' sign: If your patient is coming in after just eating a fatty meal, their gallbladder wall may appear thick from normal post prandial contraction.
I recommend continuing your biliary ultrasound learning with the lecture below as well as two great cases:
- Biliary Ultrasound Emergency Ultrasound Teaching
- UOTW Case 30 Ultrasound of the Week
- UOTW Case 8 Ultrasound of the Week
THAT'S IT FOR THIS WEEK
If you are interested in learning more about the ULA learning experience, visit their website below:

All images are courtesy of the ULA online video course. More on biliary US can be found in "Introduction to Bedside Ultrasound," Volume 1 & 2, from Dr. Mallin and Dr. Dawson. If you are interested in purchasing these ebooks for less than $1, visit Ultrasound Podcast Consumables.
Previous posts









References:
- Blaivas et al.Decreasing length of stay with emergency ultrasound examination of the gallbladder. Acad Emerg Med. 1999 Oct;6(10):1020-3.
- Young et al. Economic impact of additional radiographic studies after registered diagnostic medical sonographer (RDMS)-certified emergency physician-performed identification of cholecystitis by ultrasound. J Emerg Med. 2010 Jun;38(5):645-51.
- Kendall et al. Performance and interpretation of focused right upper quadrant ultrasound by emergency physicians. J Emerg Med. 2001 Jul;21(1):7-13.
- Ross et al. Emergency physician-performed ultrasound to diagnose cholelithiasis: a systematic review. Acad Emerg Med. 2011 Mar;18(3):227-35
- Summers et al. A prospective evaluation of emergency department bedside ultrasonography for the detection of acute cholecystitis. Ann Emerg Med. 2010 Aug;56(2):114-22.
- Ralls et al. Real-time sonography in suspected acute cholecystitis. Prospective evaluation of primary and secondary signs. Radiology. 1985 Jun;155(3):767-71.
- Ultrasound Leadership Academy Course Lectures